
If you are noticing more hair on your pillow, a wider parting, or thinning around the crown while also dealing with irregular periods, acne, weight changes, or unwanted facial hair, the issue may be more than “stress.” For many women, PCOS hair loss is one of the most emotionally difficult signs of hormonal imbalance.
Polycystic ovary syndrome is common, complex, and often underdiagnosed. The World Health Organization describes PCOS as a hormonal disorder linked with higher-than-normal androgen levels, irregular periods, abnormal ovulation, infertility, acne, excess facial or body hair, and female-pattern baldness. It affects an estimated 10–13% of reproductive-aged women, and up to 70% of affected women worldwide may not know they have it.
The good news: PCOS hair loss can often be slowed, stabilized, and sometimes partially reversed when the real driver is identified early. The key is not to treat the scalp in isolation. You need to understand the endocrine cause, check for contributing deficiencies, and choose a plan that protects both hair and long-term metabolic health.
What is Polycystic Ovary Syndrome?
Polycystic ovary syndrome, or PCOS, is an endocrine and metabolic condition that affects how the ovaries, insulin, and androgen hormones interact. It is not simply about having “cysts.” Some women with PCOS do not have obvious ovarian cysts, while some women with polycystic-looking ovaries do not have the full syndrome.
Guideline explains that PCOS diagnosis is generally based on two of three features: clinical or biochemical hyperandrogenism, ovulatory dysfunction, and polycystic ovaries on ultrasound; in adults, anti-Müllerian hormone may sometimes be used instead of ultrasound, while other causes must be excluded.
In practical terms, PCOS may affect:
- Menstrual cycles
- Ovulation and fertility
- Skin oiliness and acne
- Facial or body hair growth
- Scalp hair density
- Weight regulation
- Insulin resistance
- Type 2 diabetes and cardiovascular risk
That is why hair thinning in PCOS should not be dismissed as a cosmetic concern. It can be a visible clue that the body needs a deeper hormonal and metabolic assessment.

Common PCOS Symptoms
PCOS looks different from one person to another. Some women in Dubai come to clinic because their periods are irregular. Others come because they are struggling with acne, weight gain, fertility concerns, or thinning hair.
Common symptoms include:
- Irregular, infrequent, or absent periods
- Heavy or painful periods in some women
- Acne, especially jawline or persistent adult acne
- Oily skin
- Excess facial hair, often on the chin, upper lip, chest, or abdomen
- Scalp thinning or female-pattern baldness
- Weight gain or difficulty losing weight
- Darker, velvety skin patches in areas such as the neck or underarms
- Difficulty getting pregnant
- Mood changes, anxiety, or low confidence
PCOS is also linked with longer-term risks such as insulin resistance, type 2 diabetes, and obesity. This matters because the same insulin-androgen pathway that worsens cycles and skin symptoms can also contribute to PCOS hair loss.
How Does PCOS cause hair loss
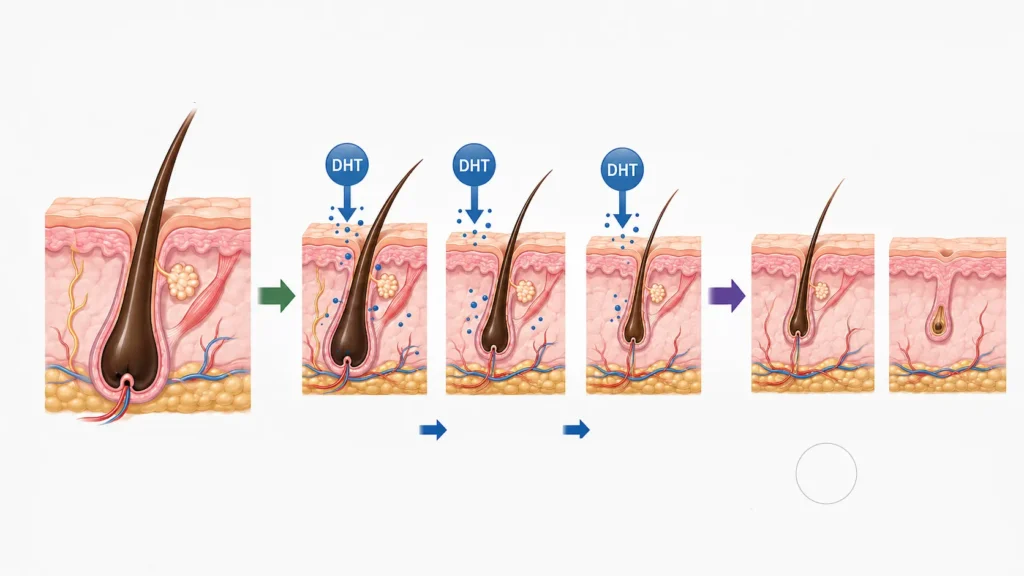
Hair follicles are sensitive to hormones. In PCOS, many women produce or respond to higher levels of androgens, including testosterone and dihydrotestosterone. These hormones can gradually shrink vulnerable scalp follicles. The result is miniaturization: hairs become finer, shorter, lighter, and less visible over time.
PCOS-related hair thinning is likely connected with increased androgen hormones and can lead to female pattern hair loss, also called androgenetic alopecia. Female pattern hair loss may accompany conditions with elevated androgen levels, including PCOS.
Several factors may overlap:
- Higher androgen levels
- Lower sex hormone-binding globulin, which can increase available testosterone
- Insulin resistance, which can amplify androgen production
- Genetic sensitivity of scalp follicles
- Iron, vitamin D, zinc, thyroid, or other nutritional factors
- Stress, crash dieting, poor sleep, or rapid weight change
- Hair breakage from heat, tight hairstyles, or harsh treatments
This is why a shampoo-only approach usually fails. The visible thinning begins at the follicle, but the trigger is often systemic.
PCOS hair loss symptoms
PCOS hair loss symptoms can be subtle at first. Many women do not see obvious bald patches. Instead, they notice a slow change in density, texture, and coverage.
Early warning signs include:
- A wider middle part
- More visible scalp under bright bathroom lighting
- Thinner ponytail volume
- Increased shedding after washing or brushing
- Short, wispy hairs that do not seem to grow long
- Thinning at the crown or top of the scalp
- Hairline changes around the temples
- More breakage because the hair shaft feels dry or fragile
Female pattern hair loss typically causes diffuse thinning from increased shedding, reduced hair volume, or both, and that it is important to distinguish it from telogen effluvium because management differs.
A practical tip!
take monthly photos in the same lighting, with the same parting, from the front, top, and sides. This makes it easier to judge whether PCOS hair loss is progressing, stabilizing, or improving.
PCOS hair loss pattern
The typical PCOS hair loss pattern is not the same as sudden patchy alopecia. It usually resembles female pattern thinning: reduced density along the part line, crown, and top of the scalp, while the frontal hairline is often partly preserved.
You may notice:
- The parting looks wider over time
- The crown looks flatter or more see-through
- Hair density decreases evenly rather than in one round patch
- The temples may thin, but complete baldness is uncommon
- Thinning is more visible when hair is wet or tied back
In PCOS, the scalp pattern often appears alongside other androgen signs such as acne, oily skin, or unwanted facial hair. That combination is a strong reason to see an endocrinologist rather than treating it as routine shedding.

PCOS vs. Male Pattern Baldness
PCOS-related thinning and male pattern baldness both involve androgen-sensitive follicles, but they do not always look or behave the same.
In male pattern baldness, hair loss often begins with a receding hairline, temple recession, and crown balding. In women, including many with PCOS, the more common pattern is diffuse thinning across the top of the scalp with a widening part. The hairline may remain present, although the density behind it becomes weaker.
The difference matters because women with hyperandrogenic symptoms need a broader medical evaluation. A clinician may assess:
- Total and free testosterone
- DHEA-S and other adrenal markers if indicated
- Menstrual history and ovulation pattern
- Thyroid function
- Ferritin and full blood count
- Vitamin D, B12, zinc, and related markers when clinically appropriate
- Glucose, HbA1c, insulin resistance risk, and lipids
Once PCOS is diagnosed, care should address reproductive, metabolic, cardiovascular, dermatologic, sleep, and psychological features, not just one visible symptom.
Is PCOS hair loss reversible?
Is PCOS hair loss reversible? The honest answer is: sometimes, partly, and usually best when treated early.
Hair follicles that are miniaturized but still active may respond to treatment. Follicles that have been inactive for a long time are harder to recover. That is why waiting years before seeking care can reduce the chance of visible regrowth.
While there is no cure for PCOS, symptoms can be managed, and hair loss due to PCOS may be improved, although it may not always return fully to its original state.
Realistic goals are:
- Reduce shedding
- Slow follicle miniaturization
- Improve scalp coverage
- Support thicker regrowth where follicles remain active
- Treat acne, excess hair growth, irregular cycles, and insulin resistance at the same time
The earlier you act, the better your odds of meaningful improvement.

PCOS hair loss before and after
When people search for PCOS hair loss before and after results, they often want reassurance that regrowth is possible. It can be, but the timeline is slower than most people expect.
A realistic timeline may look like this:
- First 6–12 weeks: shedding may continue while the plan begins working
- Around 3–4 months: early changes may appear, especially reduced shedding
- Around 6 months: better density may become noticeable if treatment is effective
- 9–12 months: photographs may show clearer improvement in coverage
- 12+ months: maintenance becomes the priority
Minoxidil-related regrowth, for example, may begin after around four months, but it often needs at least six months of consistent use and must be continued long term if effective.
For accurate PCOS hair loss before and after tracking, avoid judging progress week by week. Hair grows slowly. Use photos, shedding notes, ponytail thickness, and scalp visibility under consistent lighting.
PCOS hair loss treatment
The best PCOS hair loss treatment is personalized. A strong plan usually combines endocrine management, scalp-directed treatment, nutrition, and long-term monitoring.
- Confirm the diagnosis
Do not assume every case of thinning is PCOS. Hair loss may also come from thyroid disease, iron deficiency, postpartum shedding, autoimmune alopecia, medications, crash dieting, seborrheic dermatitis, traction alopecia, or chronic stress. - Reduce androgen impact
Depending on your goals, medical history, and pregnancy plans, an endocrinologist may discuss hormonal contraception, anti-androgen therapy, metabolic treatment, or a combination approach. The combined oral contraceptive pill is usually used to treat excessive hair growth and hair loss in PCOS. - Support follicle growth
This may include topical minoxidil, scalp care, correcting deficiencies, and treating inflammation or dandruff when present. - Treat insulin resistance and metabolic risk
Lifestyle intervention is not “just weight advice.” Insulin resistance can influence androgen levels and long-term health. The international guideline recommends a lifelong health plan with healthy lifestyle, prevention of excess weight gain, fertility optimization, and prevention or treatment of metabolic risk factors.
A complete PCOS hair loss treatment plan should be reviewed every few months, because hair response is slow and medication choices may need adjustment.

Minoxidil for PCOS hair loss
Minoxidil for PCOS hair loss is one of the most common scalp-directed options. It does not fix the hormonal cause of PCOS, but it may help follicles spend more time in the growth phase and produce thicker-looking hair.
Topical minoxidil is used for female pattern hair loss, is applied once or twice daily depending on formulation, usually requires at least six months, and may be continued long term if effective.
Important points:
- It must be applied consistently.
- Temporary early shedding can happen.
- Scalp itching or irritation may occur.
- It can cause unwanted facial hair if it drips onto the face.
- It is generally avoided during pregnancy and breastfeeding.
- If stopped, the hair may gradually return toward the pretreatment appearance.
Minoxidil for PCOS hair loss works best when the hormonal driver is also addressed. Using it without checking androgens, cycles, insulin resistance, thyroid function, or deficiencies may leave the underlying problem untreated.
Read more about Pregnancy Hair Loss: 4 Causes & Care by Dr. Ali in Dubai
Beyond Minoxidil: Anti-Androgen Medications
Anti-androgen medications reduce the effect of androgens on the hair follicle. They may be considered when there is clear hyperandrogenism, especially if hair thinning appears with acne, oily skin, or excess facial hair.
Options a specialist may discuss include:
- Combined oral contraceptive pills with lower androgenic activity
- Spironolactone
- Cyproterone-containing options where appropriate and available
- 5-alpha-reductase inhibitors such as finasteride or dutasteride in selected cases
- Metformin when insulin resistance or metabolic risk is part of the wider PCOS plan
These medicines are not suitable for everyone. Some require contraception because of pregnancy-related risks. Some require blood pressure, potassium, liver, or other monitoring. Medical management of androgenic alopecia is often more successful at slowing progression than fully reversing hair loss, and that controlling androgen overproduction in PCOS is an essential first step.
This is where endocrine expertise matters. The aim is not simply to “try tablets”; it is to choose the safest plan for your hormones, fertility goals, skin, scalp, and metabolic health.

PCOS hair loss treatment at home
PCOS hair loss treatment at home should support medical care, not replace it. Home steps can reduce breakage, improve scalp health, and support the body’s hormone environment.
Try these practical habits:
- Eat enough protein at each meal.
- Avoid crash dieting or long periods of under-eating.
- Choose high-fiber carbohydrates instead of frequent sugary snacks.
- Sleep consistently, because poor sleep can worsen appetite and insulin regulation.
- Use gentle shampooing and avoid harsh brushing when hair is wet.
- Limit tight ponytails, buns, heavy extensions, and traction styles.
- Reduce high-heat styling and aggressive chemical treatments.
- Treat dandruff, itching, or scalp inflammation early.
- Track menstrual cycles, acne flares, shedding, and weight changes.
Avoide wet brushing and tight hairstyles because they can add stress to fragile hair and increase breakage. At-home care can make the hair look and feel better, but if the parting continues to widen, you need medical assessment.
Read more about PCOS and Hair Loss: Hormonal Solutions with Dr. Ali in Dubai
PCOS hair loss supplements
PCOS hair loss supplements are popular, but they should be used carefully. More supplements do not automatically mean more growth. The right supplement depends on what your body is missing.
Commonly assessed nutrients include:
- Iron stores, usually ferritin
- Vitamin D
- Vitamin B12
- Zinc
- Folate
- Protein intake
- Omega-3 intake through food or supplements
- Myo-inositol in selected PCOS plans
complementary therapies can have variable regulation, dose, quality, consistency, and combinations with other agents.
Biotin deserves special caution. It is heavily marketed for hair, but it mainly helps when deficiency exists, and high-dose biotin can interfere with some blood tests. Before starting PCOS hair loss supplements, check labs, review medications, and choose only what supports your actual clinical picture.

The Role of Diet in Managing PCOS Hair Loss
Diet cannot “cure” PCOS, but it can influence insulin resistance, inflammation, weight regulation, and androgen activity. For many women, nutrition is a powerful foundation for PCOS hair loss treatment.
A hair-supportive PCOS plate often includes:
- Lean protein: eggs, fish, chicken, Greek yogurt, tofu, lentils, beans
- High-fiber carbohydrates: oats, quinoa, brown rice, barley, sweet potato
- Healthy fats: olive oil, avocado, nuts, seeds
- Colorful vegetables: leafy greens, peppers, carrots, tomatoes
- Iron-rich foods: lean meat, seafood, lentils, spinach paired with vitamin C
- Low-sugar drinks: water, unsweetened tea, or coffee without excess syrups
For Dubai lifestyles, the biggest challenge is often consistency: late dinners, delivery meals, sweet drinks, office snacks, and low activity during hot months. Instead of extreme restriction, focus on blood-sugar stability. Build meals that keep you full, reduce cravings, and support energy.
A useful rule!
every main meal should contain protein, fiber, and healthy fat. This supports insulin regulation and may indirectly reduce the hormonal pressure behind PCOS hair loss.
When to Seek Medical Care
Seek medical care if hair thinning is new, progressive, emotionally distressing, or happening with other PCOS symptoms. You should also book an appointment promptly if you notice:
- Sudden heavy shedding
- Bald patches
- Redness, scaling, pain, pus, or scalp sores
- Rapidly worsening facial hair or acne
- Irregular or absent periods
- Difficulty getting pregnant
- Unexplained weight gain
- Symptoms of thyroid imbalance
- Hair loss after starting a new medication
- Hair thinning before age 30
speak with a healthcare professional if hair loss is sudden, occurs with scalp redness, irritation or flaking, or is followed by pus-filled pimples on the scalp.
In Dubai, seeing an endocrinologist is especially valuable when hair loss appears with irregular cycles, acne, hirsutism, insulin resistance, thyroid symptoms, or fertility concerns. PCOS hair loss is rarely just a scalp issue.
Book your consultation with dr ali aldibbiat in dubai
If you are in Dubai and want a medical explanation for thinning hair, irregular cycles, acne, weight changes, or suspected PCOS, book a consultation with Dr Ali Aldibbiat for a structured endocrine assessment.
During a consultation, your plan may include:
- Reviewing your cycle history, symptoms, medications, and family history
- Checking androgen markers and metabolic risk
- Screening for thyroid disease and nutritional contributors
- Reviewing fertility goals before choosing medication
- Creating a safe, realistic treatment plan
- Monitoring progress over time with labs and scalp changes
For personalized care, visit Dr Ali Aldibbiat’s website and take the first step toward understanding the endocrine cause of your hair loss.

FAQs about pcos hair loss
How do you stop hair loss from PCOS?
You stop or slow PCOS hair loss by treating both the scalp and the hormonal driver. That may include confirming PCOS, checking androgen levels, managing insulin resistance, correcting iron or vitamin deficiencies, using topical minoxidil when suitable, and considering hormonal or anti-androgen medication under specialist care. The earlier treatment begins, the better the chance of stabilizing shedding.
What kind of PCOS causes hair loss?
Hair loss is most often linked with hyperandrogenic PCOS, where androgen levels are high or the follicles are very sensitive to androgens. This may appear with acne, oily skin, unwanted facial hair, irregular periods, and thinning at the crown or part line. A doctor should rule out thyroid disease, iron deficiency, adrenal causes, and other hair disorders before assuming PCOS is the only cause.
Will hair loss due to PCOS grow back?
It can improve, especially if follicles are still active and treatment starts early. Some women see reduced shedding first, then gradual thickening over several months. However, long-standing follicle miniaturization may not fully reverse. The realistic goal is to slow progression, improve density where possible, and maintain results.
What are the first signs of hormonal hair loss?
The first signs are usually a wider part, thinner ponytail, more visible scalp, increased shedding, and reduced density at the crown or top of the scalp. Hormonal hair loss may also appear with acne, irregular periods, oily skin, or excess facial hair.
What vitamins are good for PCOS hair loss?
The most relevant nutrients depend on your lab results. Iron, vitamin D, zinc, B12, folate, protein, and omega-3 intake may matter when levels are low or intake is poor. Avoid taking high-dose supplements blindly. Testing first is safer and more effective.
Conclusion
PCOS hair loss can feel frightening because it affects identity, confidence, and daily life. But it is also a signal: your body may be asking for a deeper endocrine review. Instead of buying product after product, focus on the root cause: androgen activity, insulin resistance, menstrual pattern, thyroid function, nutritional status, scalp health, and long-term metabolic risk.
The right approach is not one treatment for everyone. Some women need minoxidil. Some need anti-androgen support. Some need insulin-resistance management, thyroid care, iron repletion, or a combined plan. Many need reassurance, structure, and realistic expectations.
If you live in Dubai and suspect PCOS is behind your thinning hair, book a consultation with Dr Ali Aldibbiat. A targeted endocrine assessment can help you understand what is happening, choose evidence-based treatment, and protect both your hair and your long-term health.

